Table of Contents (click to expand)
- Is A Gunshot To The Head Instant Death?
- Location Of The Injury Is Critical
- Mass And Velocity Of The Bullet Also Determines Fatality Of The Gunshot
- Why Does A Bullet To The Head Kill So Quickly?
- How Long Can You Survive After A Gunshot To The Head?
- What Are The Chances Of Surviving A Gunshot To The Head?
- Can You Survive A Bullet To The Head?
A gunshot to the head doesn't necessarily mean instant death. Roughly 5–10% of all victims survive, and among those who reach a hospital alive, about 42% pull through. Survival depends on where the bullet enters (brainstem shots are almost always fatal; frontal-lobe and one-hemisphere hits are far more survivable), the bullet's velocity and caliber, and how quickly medical help arrives. Even when the brain itself is partly spared, blood loss is usually what kills.
Popular culture, action movies, and the media love to highlight anyone that takes a gunshot to the head and still manages to survive. Victims of gunshots are depicted in many ways, often having lost some memories, but are otherwise alive and walking around! As science aficionados, we have often scoffed at this idea. Surely, no one can survive a bullet to the head, right? Well, that’s mostly right — but survival rates are higher than many people assume. A nationwide analysis published in the Journal of Craniofacial Surgery found that among patients who reach the hospital alive, about 42% survive a gunshot wound to the head. Survival rates rise sharply based on the patient’s initial neurological condition — those with a Glasgow Coma Scale (GCS) score of 9-15 have up to a 90% survival rate, while those arriving in the worst condition (GCS 3-5) have only about an 8% chance. Overall, including victims who die before reaching medical care, roughly 5-10% of all gunshot-to-the-head victims survive.
The chance of surviving a headshot has its roots in the physics of the bullet and the biology of our bodies. Thus, a person’s odds of surviving a headshot trauma depend on the type and size of the bullet, its velocity, its trajectory, and the entry and exit point of the bullet. So, to begin, let’s try to understand the science of headshots and the aftermath of getting hit by a bullet.

Is A Gunshot To The Head Instant Death?
Not always. "Instant" death after a headshot is a real outcome, but it is not the only outcome, and which one you get depends on whether the bullet disables the parts of the brain that keep the body running second by second.
Three things have to line up for death to be genuinely instantaneous (loss of consciousness and circulation within a second or two):
- Brainstem disruption. The brainstem houses the medulla and pons, which generate the signals that drive breathing and heart rhythm. A bullet that destroys these structures stops respiratory and cardiac drive immediately. There is no recovery window, because the patient cannot breathe and the brain has no oxygen reserve to draw on.
- Massive bihemispheric or transventricular damage. Wounds that cross both cerebral hemispheres carry roughly four times the odds of dying compared with single-hemisphere wounds (Maragkos et al., 2018). Wounds that pass through the deep midline structures (the zona fatalis containing the thalamus and third ventricle) approach 100% mortality regardless of treatment.
- Catastrophic intracranial pressure spike. A high-velocity round can drive intracranial pressure above the level needed to perfuse the brain, collapsing cerebral blood flow within seconds even if the brainstem itself is anatomically intact.
If none of those happen (for example, a tangential wound that stays in one hemisphere and misses the major arteries), the victim can remain conscious for seconds to minutes, breathing on their own, with a real chance of reaching a trauma center alive. About 5-10% of all gunshot-to-the-head victims survive overall, and about 42% of those who arrive at a hospital alive go on to leave it (Journal of Craniofacial Surgery, 2023).
So the honest answer is: a headshot is usually fatal, often quickly, but it is not automatically instant. The difference between "instant" and "minutes" almost always comes down to the bullet's path through the skull.
Location Of The Injury Is Critical
The most important factor from a biological standpoint to determine survivability from a gunshot is the location where the bullet hits and passes through. The brain is a marvelous mystery, with each little cluster governing specific vital and not-so-vital functions of the body. Responsible for controlling involuntary actions, for example, the brain stem is a critical part of our body. A shot directed towards it is often fatal. The degree of injury would depend on which region the bullet penetrates through.
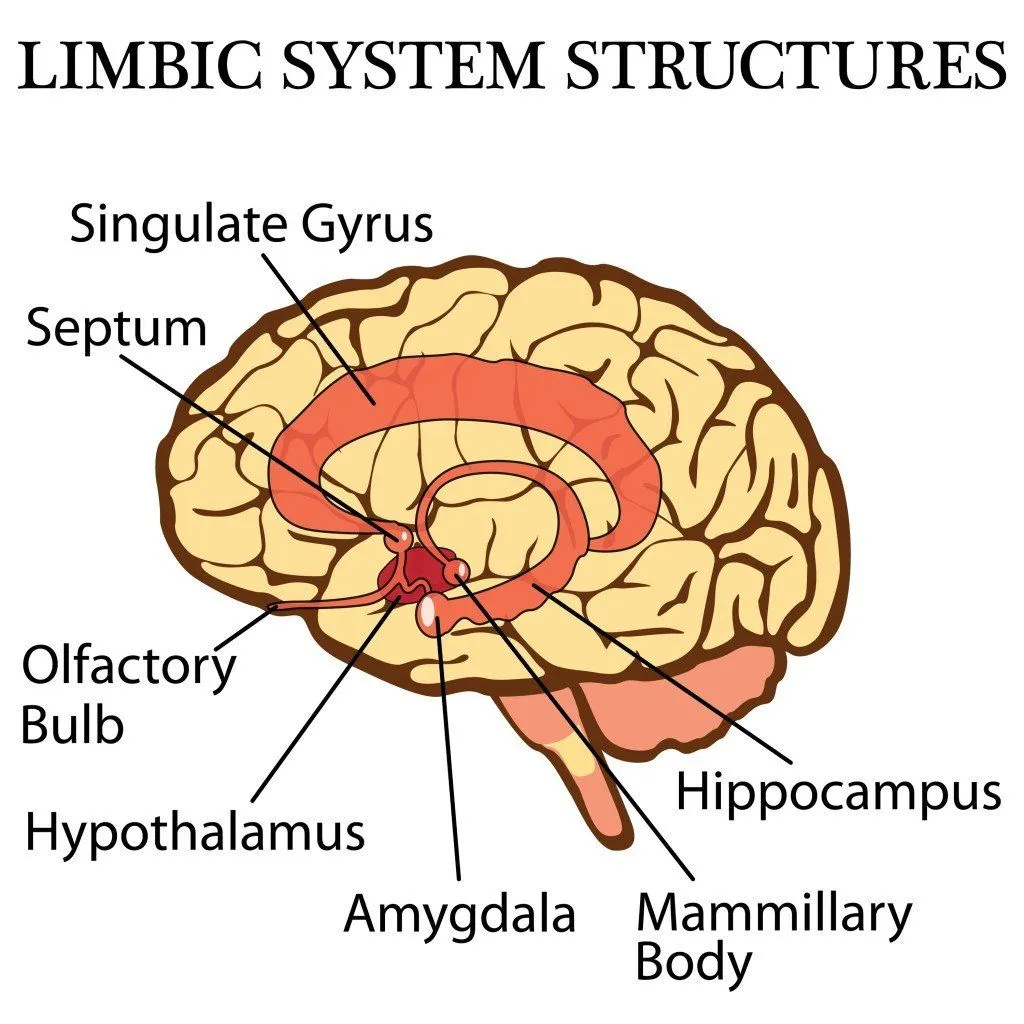
If it zips through the hippocampus — the brain's primary memory center — the injury would lead to memory loss and other memory-related problems. This is the symptom that is most commonly exploited in the daily soaps that your grandma loves so much! Damage to the amygdala affects emotional processing and fear responses, while injury to the hypothalamus disrupts hormone regulation, body temperature, and appetite. If the injury is to the frontal lobe (also seen frequently, as this is situated behind the forehead), then the survivability increases.
There is also a much greater chance of surviving a front-to-back gunshot than a gunshot received from the side. This is because, in the case of a front-to-back gunshot, it’s possible that the bullet will only damage one hemisphere of the brain, while the other is left unaffected. Our brain is a resilient organ, comparable to a twin-engine plane that can work even upon losing one engine. Major functions like cognition and speech are shared between the two hemispheres of the brain, so if one hemisphere is left intact by the bullet, the individual still has a decent chance of bouncing back from the ordeal, though never again with complete psychological and physical health.
Blood Loss After A Gunshot Proves Fatal
Since the brain stem is nestled safely at the back of the head, brain death is not usually the outright concern for the victim, but rather blood loss. The amount of blood that is potentially lost is directly influenced by the size and speed of the bullet fired. If a bullet hits any other part of the body, the impact is released to the adjoining body parts, often stabilizing the damage and saving the individual.
However, the case of the skull is unique, on account of its enclosed structure. If a high-speed bullet is fired into the skull, the skull bears the full brunt of the force, leading to skull fractures. Skull shards that pierce the brain at that point are even more difficult to remove than the bullet itself. If the skull is subjected to a high-speed, but small bullet, the worry is that the tiny bullet would ricochet around after entering the brain cavity, damaging several areas of the brain at once. The best-case scenario for survival is therefore a small, low-velocity bullet fired from a distance… with a low-caliber gun.
So far, we have discussed the gunshot mostly from a biological standpoint. Let’s now consider the fatality of the gunshot from a physics standpoint.
Mass And Velocity Of The Bullet Also Determines Fatality Of The Gunshot
From a physics standpoint, fatality would also be influenced by the kinetic energy of the fired bullet. We all know kinetic energy is given by the formula:

Here,
KE= kinetic energy
m=mass
v=velocity
This may explain why an injury inflicted by a fast-moving heavy bullet is likely to be more lethal. As we can see, the velocity of the bullet is much more crucial than the mass of the bullet, as evident from the formula. Although both mass and velocity contribute to the overall energy of the bullet’s projectile, the energy is linearly proportional to the mass, but proportional to the square of the velocity. Let’s understand this with an example: For a constant velocity of a bullet, if the mass is doubled then the resultant kinetic energy is also doubled. But on the other hand, for the constant mass of the bullet if the velocity is doubled, then the energy increase quadruples i.e. increases four times.

As you can see, fatality and time to death would heavily depend on the velocity of the bullet. The velocity of the bullet, in turn, depends on the firearm being used. For example, a bullet shot from the lethal AK-47 rifle has a very high speed. They are infamous for inflicting severe peripheral damage to the critical regions in the brain as they pass through, as compared to relatively slower-moving bullets from a handgun.

The US military conventionally uses 5.56mm bullets, which have a comparatively lower mass than a typical bullet, but move really quick. As a result, they produce much more kinetic energy, which is then transmitted to the tissues of the target, causing them to rupture.
Why Does A Bullet To The Head Kill So Quickly?
A bullet to the chest can kill, but usually over minutes through blood loss. A bullet to the head can kill in a fraction of a second. Three biological facts explain the speed.
The brain runs the body in real time. The brainstem (specifically the medulla and pons) generates the signals that drive each breath and each heartbeat. Lung tissue, heart muscle, and blood vessels can all function for hours without nerve input, but they cannot start themselves. When a bullet disrupts the brainstem, respiration ceases within the same second, and circulation follows shortly after. There is no equivalent of CPR for an absent respiratory center.
The brain has almost no metabolic reserve. Neurons consume roughly 20% of the body's oxygen and glucose despite making up only about 2% of body weight, and they store almost none of it. Once cerebral blood flow stops, ATP is exhausted within seconds, and the ischemic cascade (membrane depolarization, calcium influx, glutamate-driven excitotoxicity) kills cells over the next few minutes. This is the same mechanism that makes untreated strokes catastrophic.
The skull is a closed box. When a high-velocity round enters, the temporary cavity it carves produces pressure spikes that have been measured at up to 30 atmospheres (around 440 psi) in ballistic-gel and brain-simulant studies. The skull cannot expand to absorb that pressure, so the energy is dumped into brain tissue, and the resulting swelling has nowhere to go. Intracranial pressure climbs, cerebral perfusion pressure falls, and the brain begins to suffocate even without further damage from the bullet itself.
Take any one of those away (brainstem spared, blood flow preserved, pressure controlled by emergency surgery), and the picture changes from "minutes to die" to "minutes to save."
How Long Can You Survive After A Gunshot To The Head?
The honest answer depends on whether the brainstem stays online. If it does, there is usually a window of minutes (and sometimes hours) before death. If it doesn't, that window can be measured in seconds.
When a bullet enters the skull, two injury patterns unfold at once. The projectile carves a permanent wound channel through brain tissue, while the pressure waves radiating outward from its path stretch and tear tissue several centimeters beyond that channel, creating a transient temporary cavity. Peak pressures inside this cavity have been measured at up to 30 atmospheres (around 440 psi) in ballistic-gel and brain-simulant studies, which is enough to rupture neuronal membranes and seed scattered hemorrhages well outside the visible wound track.
A rough timeline of what happens after impact:
- First few seconds. If the bullet disrupts the brainstem, where the centers that drive breathing and heart rate live, loss of consciousness is essentially instantaneous and breathing usually stops at the same moment. If the brainstem is spared but cerebral blood flow drops sharply (from massive bleeding or a sudden spike in intracranial pressure), a 2016 scoping review of 39 human and animal studies found that clinical loss of consciousness and loss of EEG activity occur within roughly 30 seconds of abrupt circulatory arrest.
- First few minutes. Brain tissue holds almost no energy reserve. Once cerebral blood flow stalls, neurons begin consuming their available ATP within seconds, and oxidative phosphorylation collapses soon after. The ischemic cascade that follows (membrane depolarization, potassium leaking out, calcium and sodium flooding in, glutamate-driven excitotoxicity) is the same one that kills cells in untreated stroke, and it produces irreversible neuronal injury within minutes.
- 30 minutes to several hours. Even when the patient is breathing and has a pulse, cerebral edema (brain swelling) starts measurably as early as 30 minutes after the injury. Inside the closed box of the skull, swelling pushes intracranial pressure up. Once intracranial pressure climbs above roughly 20-25 mmHg, or cerebral perfusion pressure falls below about 60 mmHg, the brain begins to suffocate even though the bullet is no longer doing fresh damage. This is the window in which fast prehospital care and emergency neurosurgery actually save lives.
- Days to weeks. In survivors, the danger doesn't end in the operating room. Roughly half develop post-traumatic seizures, in-driven bone and scalp fragments raise infection risk, and rehabilitation arcs are measured in months to years.
The takeaway: "instant" death after a headshot is real, but it requires the bullet to either take out the brainstem or destroy enough of both hemispheres for blood pressure to collapse outright. Wounds that spare the brainstem and miss major vessels can leave a victim conscious for several minutes, and that narrow window is exactly the one emergency neurosurgeons are trained to exploit.
Are You Conscious After Being Shot In The Head?
It depends on what the bullet hits in the first instant.
If the bullet disrupts the brainstem, loss of consciousness is effectively simultaneous with the shot. The reticular activating system, which keeps you awake, runs through the upper brainstem, so disrupting it switches awareness off the way a power cut switches off a light. There is no perceived pain, no last thoughts, no fading.
If the brainstem is spared but cerebral blood flow collapses (because the bullet tore a major artery, or because intracranial pressure has spiked enough to stall perfusion), the picture is less abrupt. The 2016 scoping review by Brodbelt and Stoodley cited above found that clinical loss of consciousness and loss of EEG activity occur within about 30 seconds of abrupt circulatory arrest. Some survivors of self-inflicted gunshot wounds, including Christen McGinnes (whose case is described in the next section), have reported being conscious immediately after the shot and able to call for help.
If the wound spares both the brainstem and the major vessels, a victim can stay alert for several minutes. That window is the one emergency neurosurgeons are racing to exploit.
What Are The Chances Of Surviving A Gunshot To The Head?
This is the question search engines see most often, and the honest one-line answer is that survival depends on three things: the patient's neurological condition on arrival, the path the bullet took through the brain, and whether it damaged major vessels. Each of those swings the odds substantially.
The single most useful clinical predictor is the SPIN score (Survival after acute civilian Penetrating brain Injuries), developed by neurologist Susanne Muehlschlegel and colleagues from a cohort of 413 patients at the University of Maryland and the University of Massachusetts. The SPIN score combines admission Glasgow Coma Scale motor subscore, pupillary reactivity, Injury Severity Score, sex, transfer status, INR (a blood-clotting marker), and whether the wound was self-inflicted, into a single number from 4 to 52, with higher scores predicting higher survival. It achieved an area under the ROC curve of 0.96 in the original cohort and 0.88 in an independent multicenter validation, which is unusually strong discrimination for a trauma scoring tool.
The bullet's path matters almost as much as the patient's GCS. A 2018 meta-analysis pooling 1,774 civilian patients (Maragkos et al., Journal of Neurotrauma) identified two trajectory features that worsen outcomes sharply:
- Bihemispheric wounds (the bullet crosses from one cerebral hemisphere into the other) carry roughly four times the odds of dying compared with wounds that stay in one hemisphere (odds ratio 4.23, 95% CI 2.32-7.68).
- Multi-lobar wounds (passing through several lobes within a hemisphere) carry roughly six and a half times the odds of dying (OR 6.53, 95% CI 1.99-21.42).
Even more dramatically, wounds that pass through what neurosurgeons call the zona fatalis, the deep midline region containing the third ventricle, hypothalamus, and thalamus, have nearly 100% mortality regardless of treatment. The radiology sign of a bullet track crossing the ventricles in both directions (the "tram-track" sign on CT) is, in current civilian practice, almost universally fatal.
Pulled together, the by-the-numbers summary looks like this:
- Overall, including victims who never reach a hospital: 70-90% die before arrival, and roughly half of those who do reach the ED die there. Of the entire population of headshot victims, only about 5-10% survive.
- Among patients who reach a hospital alive: about 42% survive (Journal of Craniofacial Surgery, 2023).
- By admission GCS: roughly 90% of those arriving with GCS 9-15 survive; only about 8% of those arriving with GCS 3-5 do.
- By trajectory: unilateral, single-lobe wounds are the most survivable; bihemispheric, multi-lobar, and transventricular paths are the least.
- By age: children fare meaningfully better than adults at every comparable severity. Bihemispheric wounds carry roughly 82% mortality in adults versus about 60% in children.
- By intent: self-inflicted GSWs to the head are about 90% fatal versus around 25% for assault-related GSWs (discussed further in the next section).
None of these numbers are destiny. The authors of the SPIN paper explicitly warn against using their own score to drive individual treatment-withdrawal decisions, because a small but real fraction of patients with apparently catastrophic presentations recover, which is why most US trauma centers now resuscitate aggressively first and re-assess later.
Can You Survive A Bullet To The Head?
As mentioned earlier, blood loss is the real villain in such scenarios, but there is a window of a few minutes wherein the victim can remain conscious and survive. If the victim immediately receives medical attention during this time, there is a better chance of avoiding an untimely end.

Neurosurgeons opine that victims stand a chance to survive a headshot if they can continue breathing and their blood pressure does not drop too much. Both functions are essential to ensure an adequate supply of oxygen to the brain in this exigency. Upon the arrival of medical aid, the doctors can try their best to remove the dead tissue and clear the area to relieve the imminent swelling. Otherwise, the swelling will have no outlet and begin to come out at the base, which often has fatal consequences. Sometimes, doctors place drains to remove excess fluids and avert this type of dangerous brain-swelling.
Treatment of gunshot wounds to the head has advanced significantly. Updated guidelines from the Brain Trauma Foundation emphasize that even severe penetrating brain injuries can have good outcomes with prompt management. Modern neurosurgeons now use endovascular techniques to treat traumatic pseudoaneurysms (damaged blood vessels), which are often superior to open surgery. Monitoring optimal cerebral perfusion pressure (CPPopt) has also become an important tool in post-injury care. About 50% of surviving patients will develop seizures and require long-term anti-epilepsy medication, and most survivors need extended rehabilitation.
Case Study Of Christen McGinnes: Remarkable Story Of A Headshot Survivor
Self-inflicted gunshot wounds to the head are significantly more lethal than those from assaults — roughly 90% of self-harm GSWs to the head are fatal, compared to about 25% of assault-related head GSWs. This makes the following survival story all the more remarkable.
In 2016, The Trace, a non-profit gun-specific news portal published a story of Christen McGinnes, who survived a self-inflicted gunshot wound in her suicide attempt in 2009. She narrated her remarkable story of miraculously surviving a deliberate gunshot to her head to end her life.
During the subprime crisis in 2009, Christen, a woman in her 40s, was fired from a job, lost her close kin and even her pet dog passed away. It was the peak of the financial crisis of 2009 and she was running out of savings in such challenging times. On one particularly fateful night in 2009, she loaded her 0.357 revolver with hollow-point bullets and placed the gun underneath her chin, a shot that she felt would result in instant death.
She pulled the trigger and while she blew off much of her face, lost many teeth, charred her tongue and lost an eye, she miraculously survived. She was immediately rushed to Fairfax Inova Hospital by her neighbors, where she was treated. She had to undergo several surgeries and was in semi-coma state for a number of weeks in the hospital. Her face was distorted and she couldn’t eat or speak without aid for a long time. It was only after a few years that she could talk again and narrate her remarkable story of surviving the suicide attempt.
So, as you can see, there is a chance—albeit a very slim one—to survive a gunshot to the head. However, the aftermath of surviving a gunshot is scary. As in the case of Christen, she ended up losing more than half of her teeth, one-third of her tongue and half her vision. No patient can come out of such a terrible injury unscathed, which is why gun violence remains a critical public health issue. In the United States alone, over 44,000 people died from gun violence in 2024, according to CDC data — though this represented a 7% decline from the previous year. Responsible access to firearms is a critical issue that must be addressed in our modern world.
References (click to expand)
- Muehlschlegel, S., Ayturk, D., Ahlawat, A., Izzy, S., Scalea, T. M., Stein, D. M., … Sheth, K. N. (2016, October 26). Predicting survival after acute civilian penetrating brain injuries. Neurology. Ovid Technologies (Wolters Kluwer Health).
- Cranial GunShot Wounds - UCLA Neurosurgery, Los Angeles, CA - neurosurgery.ucla.edu:80
- Neurosurgical Treatment for Gunshot Wound Head Trauma. The American Association of Neurological Surgeons
- . (2004). Firearms and Violence. []. National Academies Press.
- A Nationwide Analysis of Gunshot Wounds of the Head. Journal of Craniofacial Surgery (2023).
- Gunshot wound to the head not a death sentence. Yale School of Medicine.
- Penetrating Brain Injury: Good Outcomes Achievable Even in Grave Cases. Cleveland Clinic.
- What the data says about gun deaths in the US. Pew Research Center (2025).
- Hippocampus: What It Is, Function & Damage. Cleveland Clinic.
- Penetrating Head Trauma. StatPearls. NCBI Bookshelf.
- Brodbelt, A., & Stoodley, M. (2016). Time to loss of brain function and activity during circulatory arrest. Journal of Critical Care.
- Circulatory Arrest, Brain Arrest and Death Determination. Frontiers in Cardiovascular Medicine (2018).
- Maragkos, G. A., Papavassiliou, E., Stippler, M., & Filippidis, A. S. (2018). Civilian Gunshot Wounds to the Head: Prognostic Factors Affecting Mortality: Meta-Analysis of 1,774 Patients. Journal of Neurotrauma.
- Multicenter Validation of the Survival After Acute Civilian Penetrating Brain Injuries (SPIN) Score. PMC.